Alcor’s long-term planning is fiscally conservative. Any excess funding also goes toward long-term care unless the member specifies otherwise. As a result, Alcor has more funding set aside per volume of patients under care than any other organization by a wide margin.
Alcor also segregates long-term care funds in the Patient Care Trust (PCT), which has a separate board of directors that oversees investments and ensures PCT funds are only used for long-term patient care. No other cryonics organization has this structure.
Alcor attempts to provide bedside standby service to all members in the U.S. and Canada. The purpose of standby is to begin stabilization and transport procedures immediately after clinical death, which is critical for an optimal outcome.
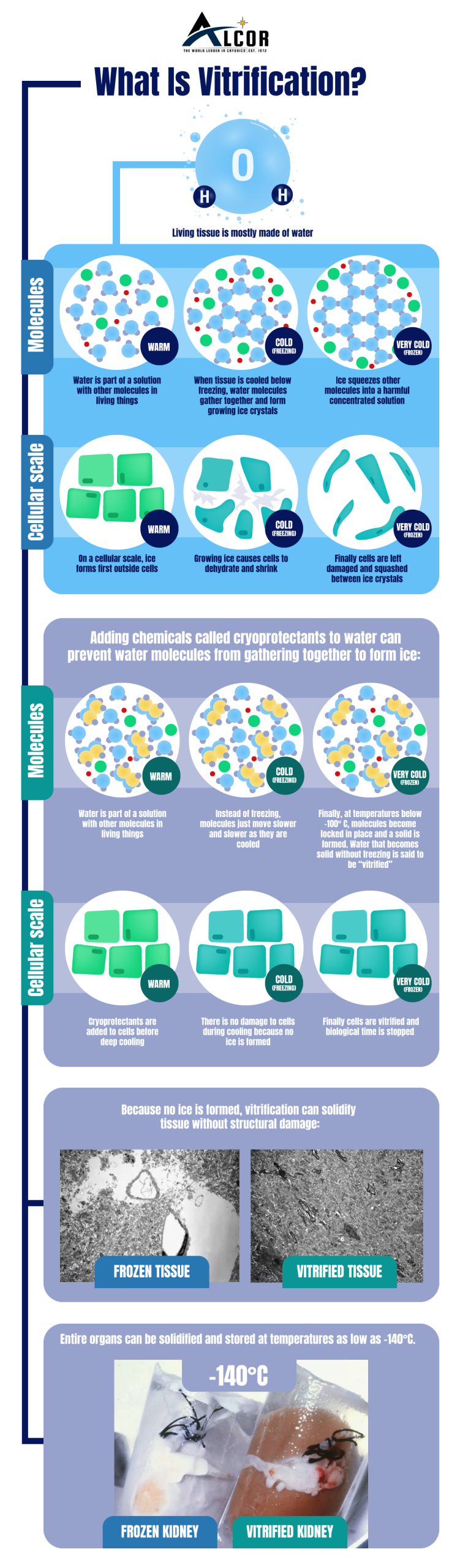
Alcor uses cryopreservation technology and solutions developed for medical applications by leading cryobiology researchers. The M22 vitrification solution used by Alcor is the product of decades of research in mainstream laboratories working to cryopreserve whole organs for organ banking. It incorporates numerous patented technologies that prevent ice formation, reduces toxicity, and eliminate chilling injuries. It was the first solution to ever permit the cryopreservation and subsequent long-term survival of a vital mammalian organ (kidney). M22 is a “6th generation” vitrification solution, incorporating ice blockers, chilling injury protection, and numerous other insights.
Alcor uses “closed circuit” perfusion, the same method of circulating fluids through the body used in heart surgery and organ cryopreservation research. This permits cryoprotectant to be introduced more gently, with better temperature control.
Learn more here!