Whole Body or Neuropreservation
Alcor offers two core pathways:
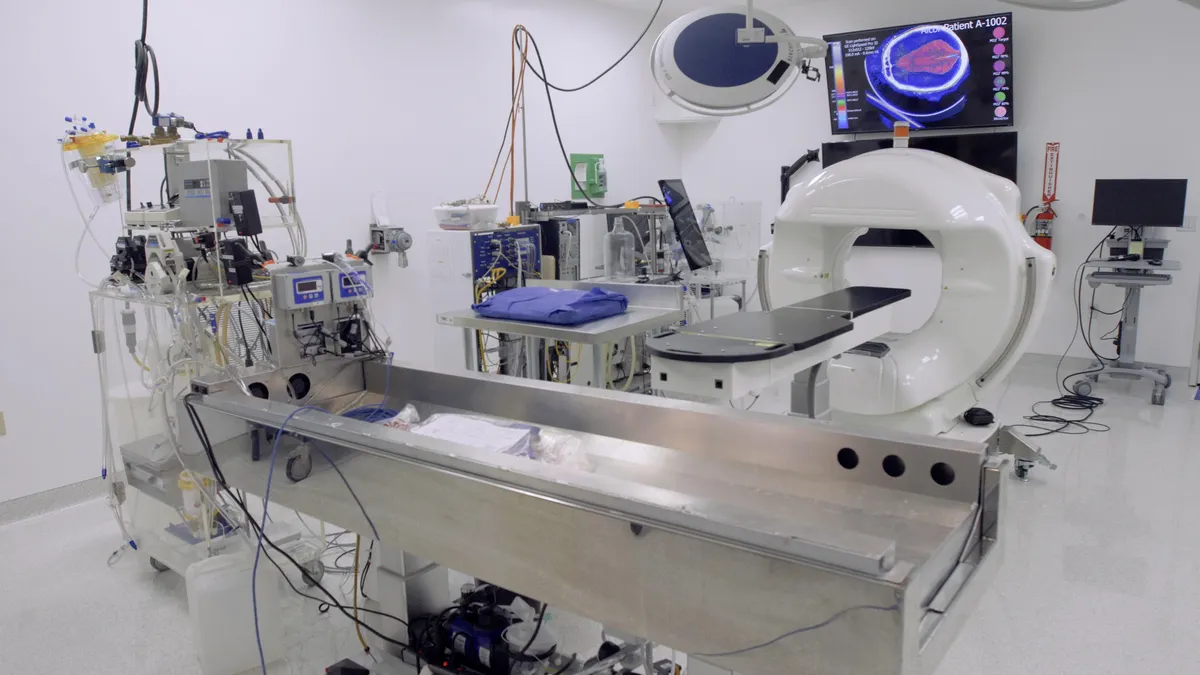
Whole‑body cryopreservation keeps your entire anatomy intact for future medicine that may be able to repair and rejuvenate every organ and tissue.
Neuropreservation concentrates resources on the brain, the seat of memory and identity, assuming tomorrow’s technology can provide a healthy new body.
While the choice of procedure is solely up to the member, both options share the same rapid‑response timeline and long‑term care.
Learn About Deployment & Recovery